Approved for patients ages 12 years and older. Click here for different pediatric patient dosing.
//
CLINICAL STUDIES
Significant improvements in skin clearance and itch relief with Adbry
Kalvin, a real Adbry patient. Individual results may vary.
EASI, IGA and Pruritus NRS at Week 16
Significant improvements in skin clearance, lesion extent and severity with both monotherapy and combination therapy 1,3
Additional Clinical Results


//
BASELINE CHARACTERISTICS
Adbry was extensively studied in 3 robust pivotal trials
The efficacy and safety of Adbry were assessed in 3 randomized, double-blind, placebo-controlled trials1
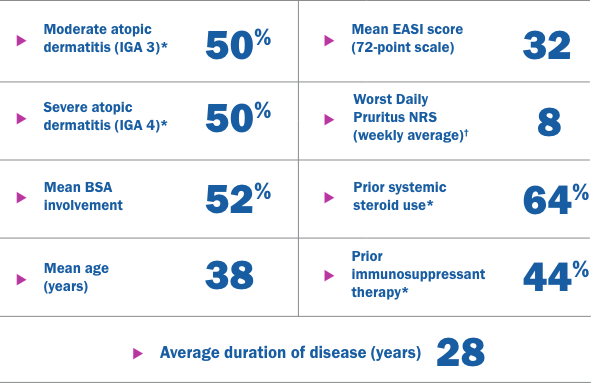
Adbry was assessed as monotherapy and as combination therapy (with TCS as needed)
Primary Endpoints1
- Improvement of at least 75% in EASI (EASI-75) at Week 16
- Achievement of IGA 0 or 1 (clear or almost clear skin) at Week 16
Secondary Endpoint1
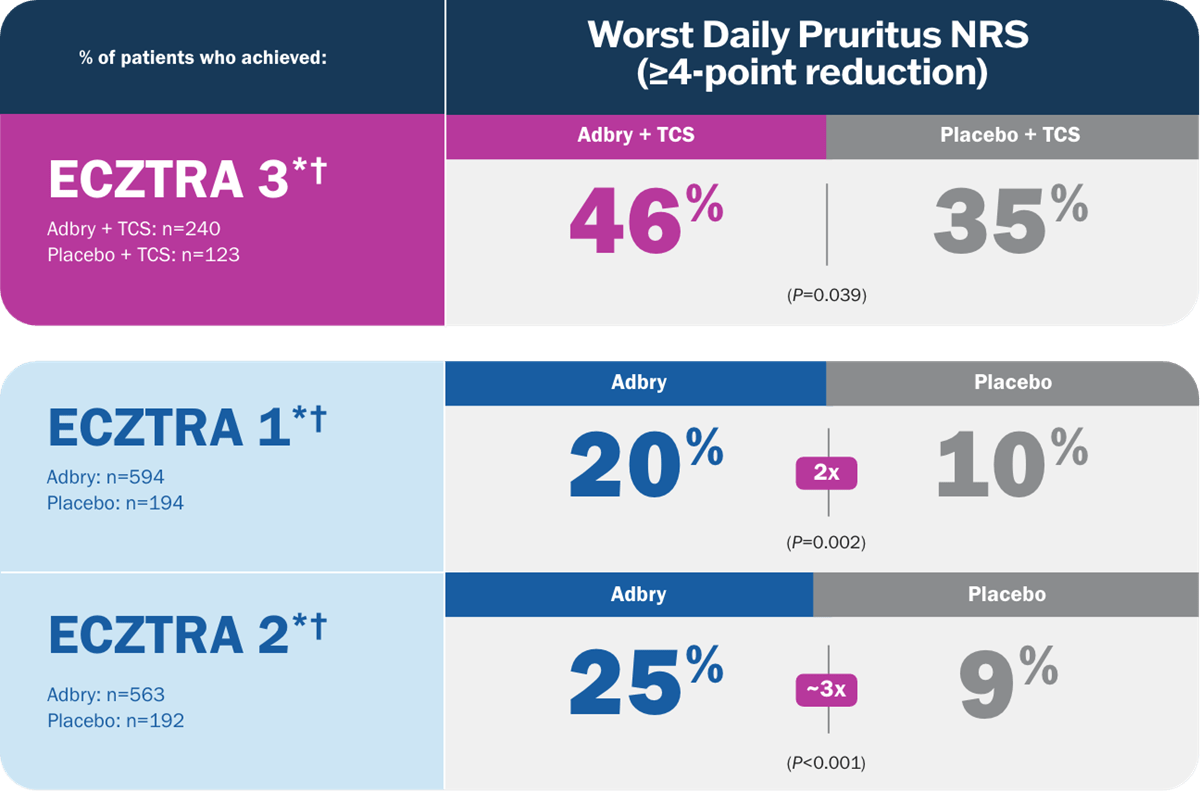
- Reduction of Worst Daily Pruritus NRS (weekly average) of at least 4 points on the 11-point itch NRS from baseline to Week 16
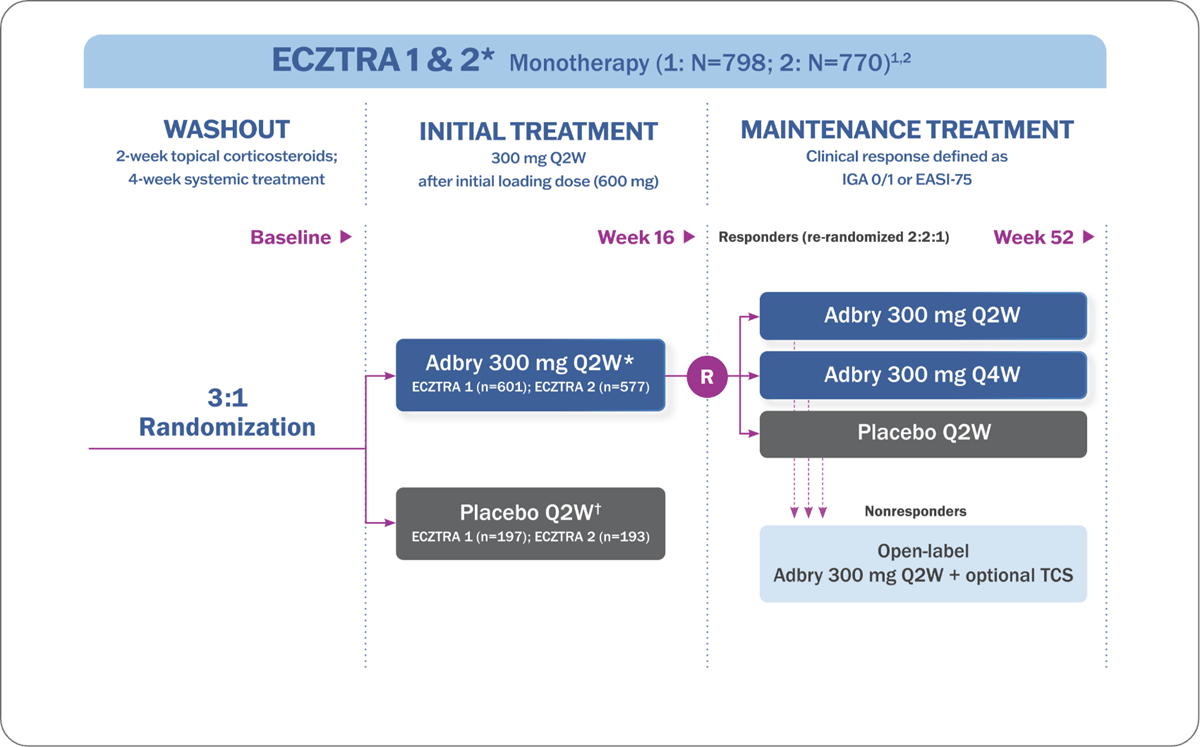
Q2W=every 2 weeks; Q4W=every 4 weeks; TCI=topical calcineurin inhibitor; TCS=topical corticosteroid.
Adbry was administered via subcutaneous injection.
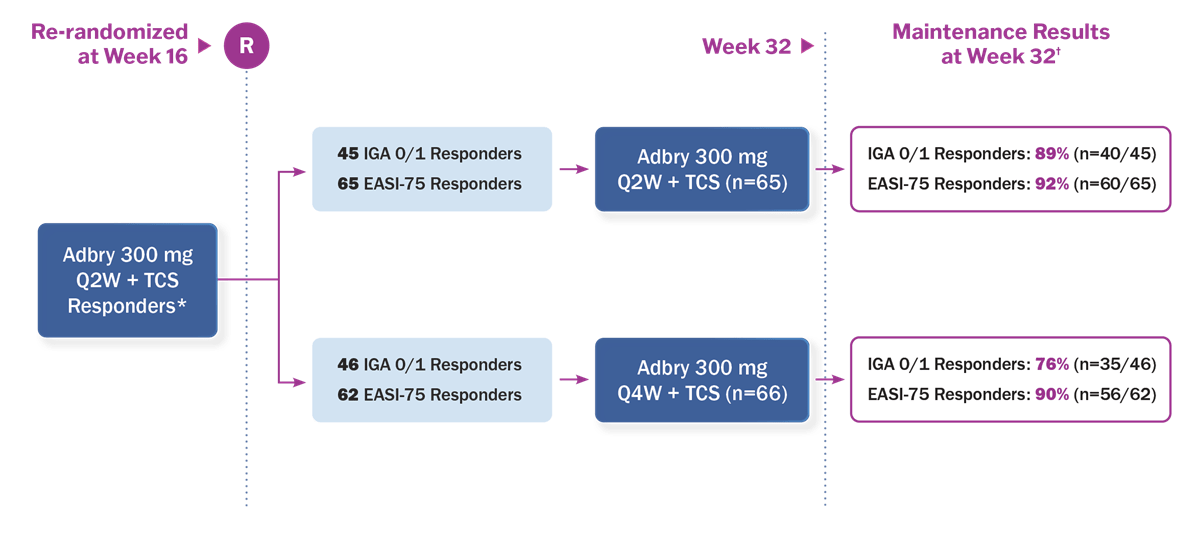
*Responders defined as achieving the primary endpoints of IGA 0 or 1 or EASI-75 at Week 16.
Nonresponders at Week 16 and subjects who lost clinical response during the maintenance period were placed on open-label treatment with Adbry 300 mg every other week and optional use of TCS.1
†Placebo responders continued on placebo to maintain blind participation and were not included in analyses after Week 16.1,2
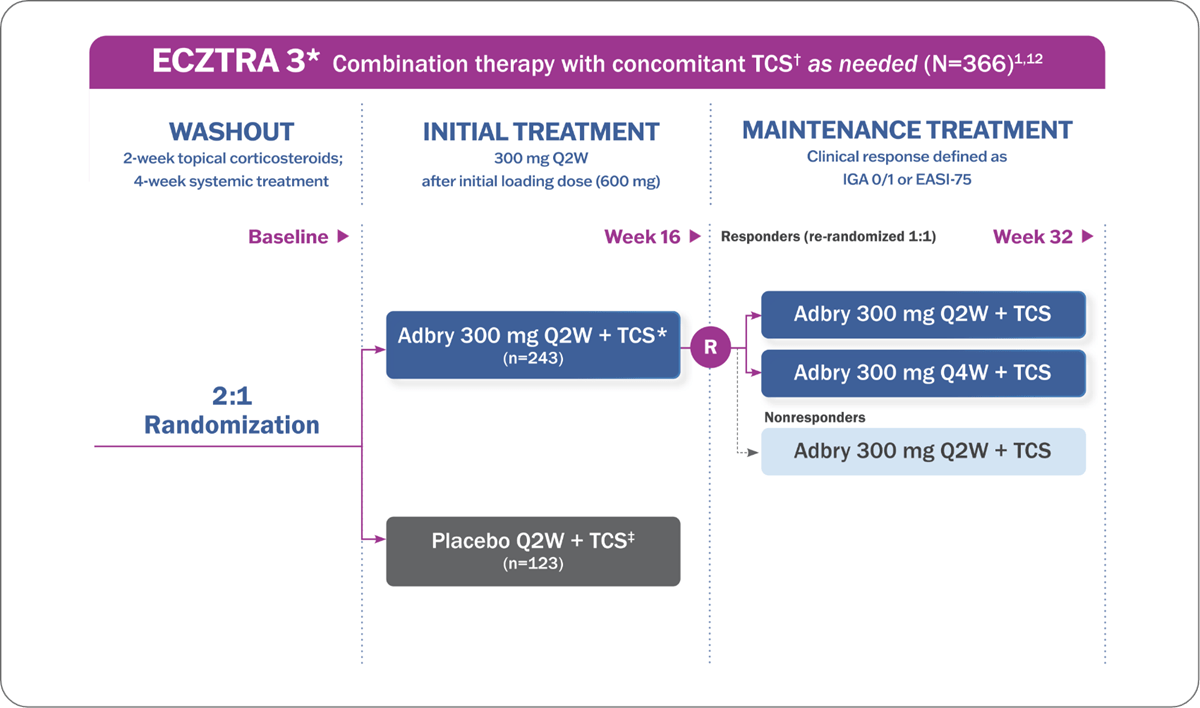
Adbry was administered via subcutaneous injection.
*Responders defined as achieving the primary endpoints of IGA 0 or 1 or EASI-75 at Week 16. Subjects who did not achieve clinical response at Week 16 received Adbry 300 mg every other week+TCS for another 16 weeks.1,3
†A midpotency TCS (ie, mometasone furoate 0.1% cream) was dispensed at each dosing visit. The subjects were instructed to apply a thin film of the dispensed TCS as needed, once daily, to active lesions from Week 0 to Week 32, and were to discontinue treatment with TCS when control was achieved. An additional, lower-potency TCS or TCI could be used at the investigator’s discretion on areas of the body where use of the supplied TCS was not advisable, such as areas of thin skin.
‡Placebo responders continued on placebo to maintain blind participation and were not included in analyses after Week 16.1,2
//
EASI & IGA
Adbry demonstrated significant improvements in skin clearance and lesion extent and severity1,3
- Significantly more patients achieved the primary endpoints of EASI-75 and IGA 0/1 at Week 16 with Adbry + TCS vs placebo + TCS
- In monotherapy trials, 2x to 3x as many patients treated with Adbry vs placebo achieved improvements in the primary endpoints of EASI-75 and IGA 0/1 at Week 16
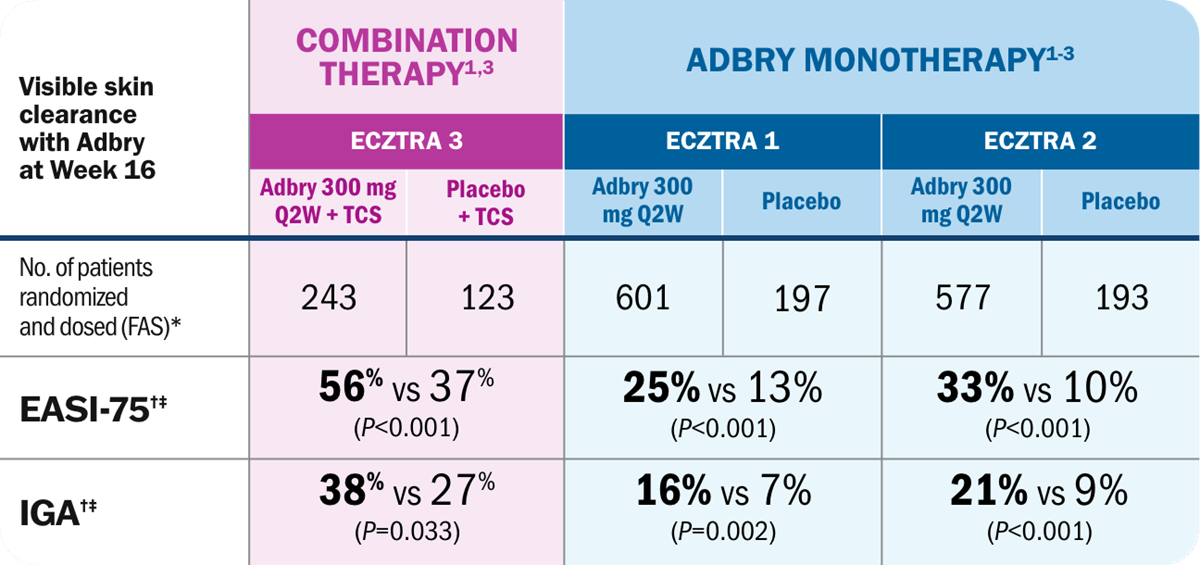
*Full Analysis Set (FAS) includes all subjects randomized and dosed.
†Subjects who received rescue treatment or with missing data were considered nonresponders.
‡Percentage of patients who achieved response.
Visible improvements you can see at 16 weeks
Improvement in atopic dermatitis lesions at Week 16
ADBRY MONOTHERAPY Q2W2


BEFORE TREATMENT
EASI = 31.9
IGA = 4
Worst Daily Pruritus NRS = 8
AT WEEK 16
EASI = 3.6
IGA = 2
Worst Daily Pruritus NRS = 3
Example of improvement in EASI from baseline to Week 16 in a patient receiving Adbry in the ECZTRA 2 study.3 Individual patient results may vary.
Topical corticosteroid use (as needed) with Adbry at Week 163
Not actual size
ECZTRA 3: COMBINATION THERAPY
Patients (%) who used ZERO OR MINIMAL (0 to <5 g) of supplied TCS over the last 2 weeks of the initial 16-week treatment period (adjusted mean):
Amount of TCS used over the last 2 weeks of the initial 16 week treatment period (adjusted mean)*
*Assuming no TCS used from the nonreturned tubes during the initial treatment period. Data collected after permanent discontinuation or initiation of rescue medication not included.
Limitations:
Analyses of TCS use as needed were based on the provided TCS only (mometasone furoate 0.1% cream provided every other week applied once daily as needed). Additional low potency TCS and TCI were allowed as needed and not accounted for in this analysis. Analyses were prespecified but not adjusted for multiplicity. Conclusions should be made with caution.
//
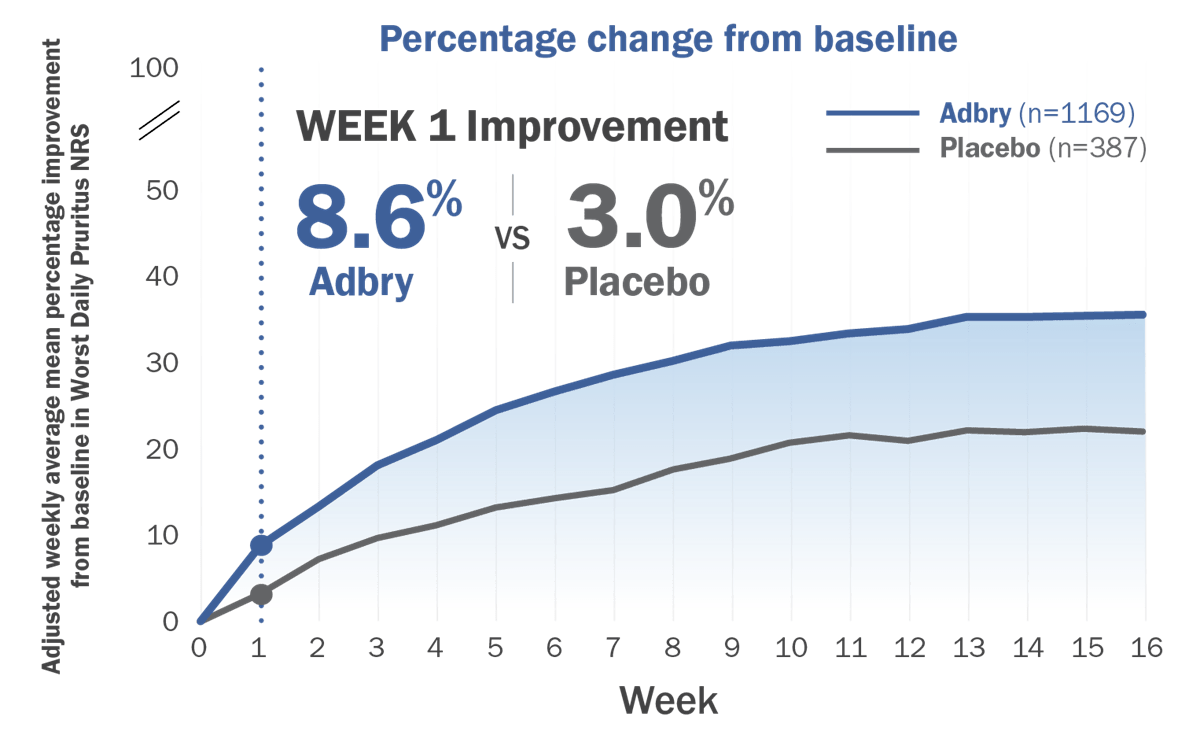
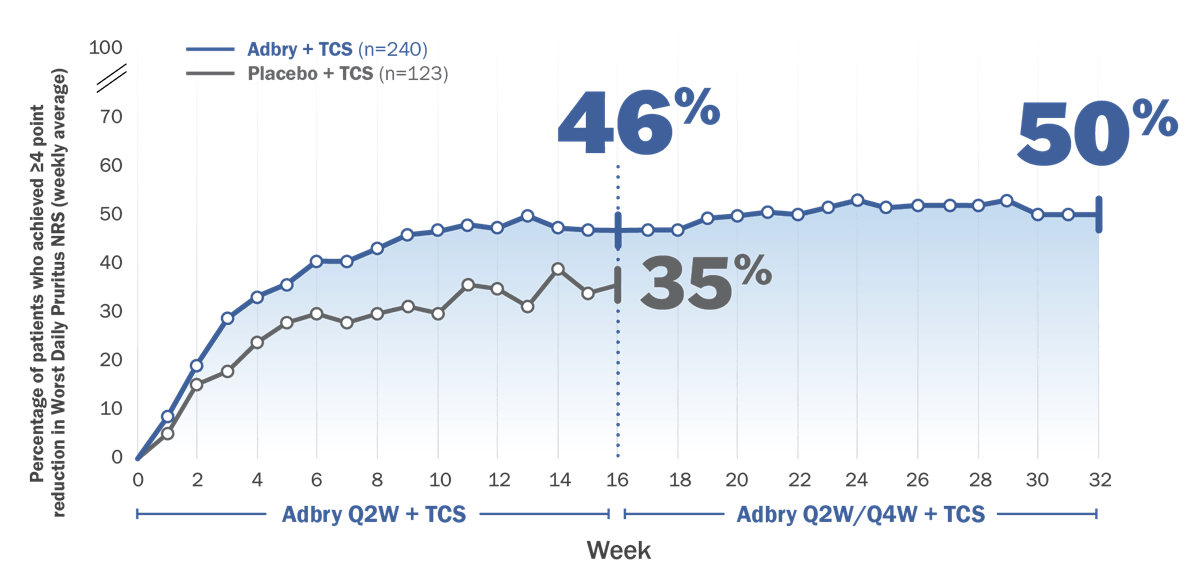
WORST DAILY PRURITUS (NRS)
Adbry itch response data

Beth, a real Adbry clinical trial patient. Individual results may vary.

//
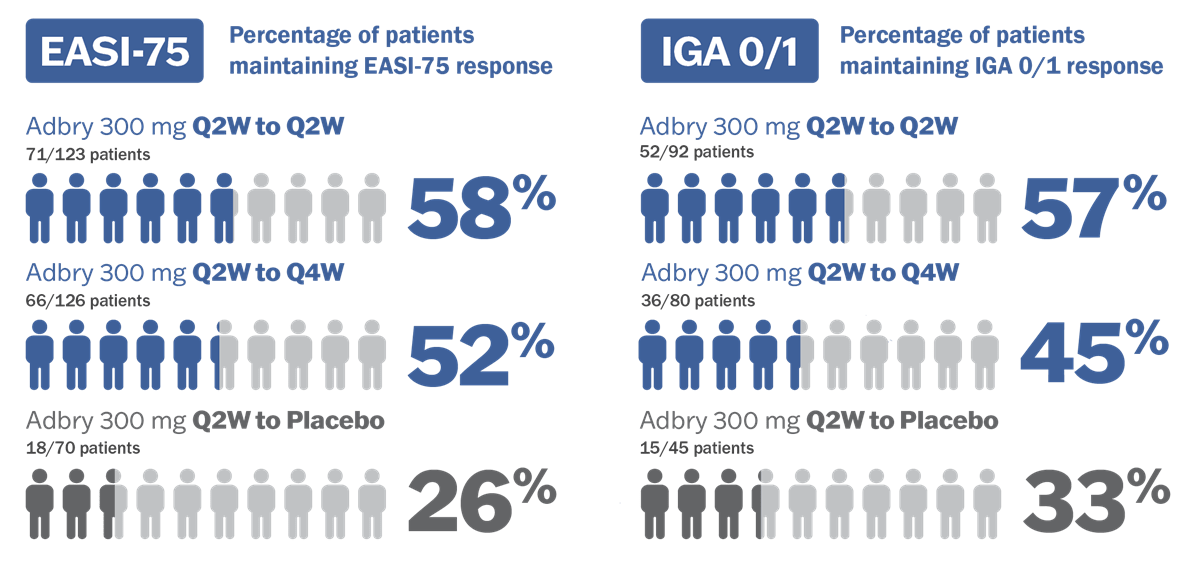
MAINTENANCE OF RESPONSE
With Adbry, achieve lasting disease control for your patients at Week 32 and Week 521
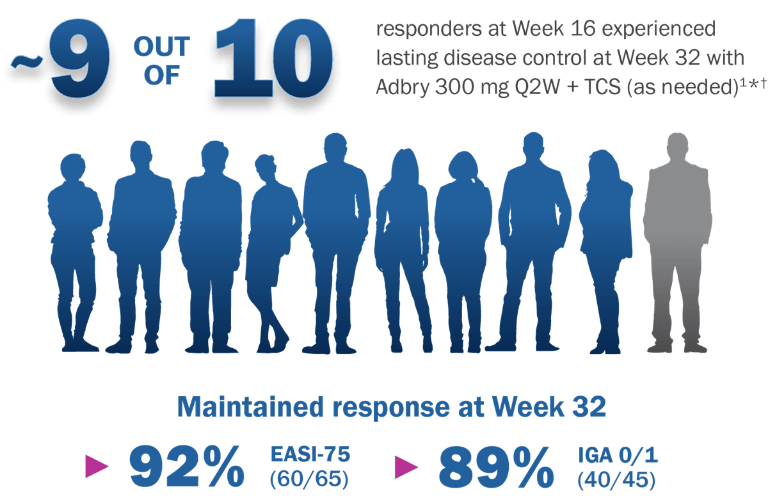
ECZTRA 3 study diagram:
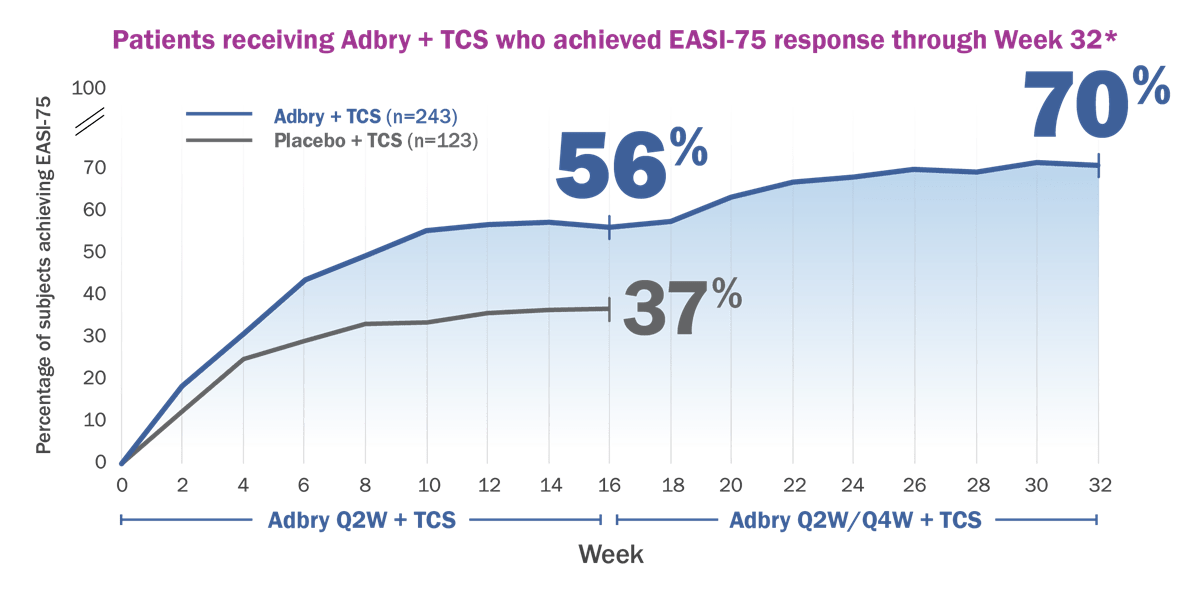
Analysis of patients achieving EASI-75 at Week 323*
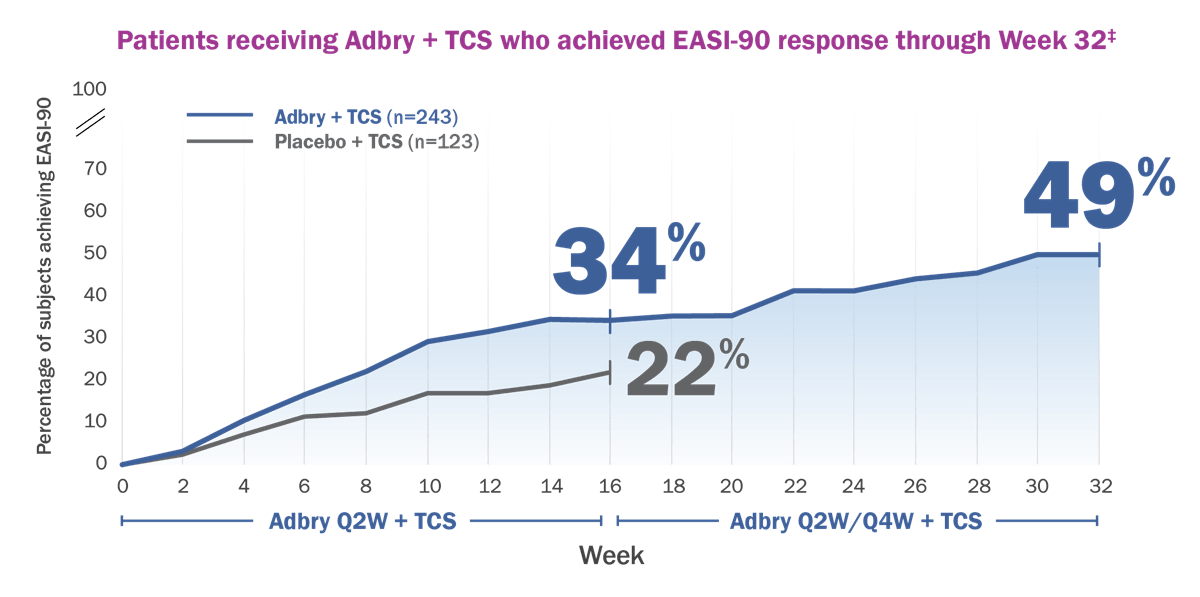
EASI-90 improvement through 32 weeks with Adbry + TCS (as needed)3
Itch reduction with Adbry + TCS (as needed)3
See lasting control with Adbry monotherapy Q2W or Q4W3
Not an actual size
In ECZTRA 1 and 2,
MORE THAN HALF OF RESPONDERS
at Week 16 maintained response at Week 52
with Adbry 300 mg Q2W as monotherapy without any TCS use in a pooled analysis3*†
Q2W=every 2 weeks; Q4W=every 4 weeks; TCS=topical corticosteroid.
*Responders were defined as subjects with an IGA 0 or 1 (“clear” or “almost clear”) or EASI-75 at Week 16. At Week 16, responders were re-randomized to Adbry 300 mg Q2W, Adbry Q4W, or placebo every other week for another 36 weeks.
†Subjects who received rescue treatment or with missing data were considered nonresponders.
//
OPEN-LABEL EXTENSION RESULTS
The ECZTEND OLE (Open-Label Extension) trial results up to 3 years
The ECZTEND OLE trial is an ongoing long-term assessment of safety and efficacy4
- The ECZTEND study is an ongoing, 5-year, single-arm, open-label, long-term extension trial. Patients were permitted to enter ECZTEND after completion of the Adbry parent trials and a skin-barrier function study, regardless of treatment response or whether they were treated with Adbry or placebo. Patients received a 600 mg loading dose followed by 300 mg Q2W + optional TCS (as needed)
- Patients in the 3-year efficacy cohort were treated with Adbry (Q2W or Q4W monotherapy or Q2W + optional TCS [as needed] in parent trials ECZTRA 1 and 2 open-label arm) for 52 weeks in parent trials ECZTRA 1 and 2, followed by up to 104 weeks of treatment in ECZTEND
- This safety analysis cohort includes patients from parent trials ECZTRA 1, 2, 3, 4, 5, and 7 (n=1,430) as of data cutoff, regardless of duration of treatment exposure3
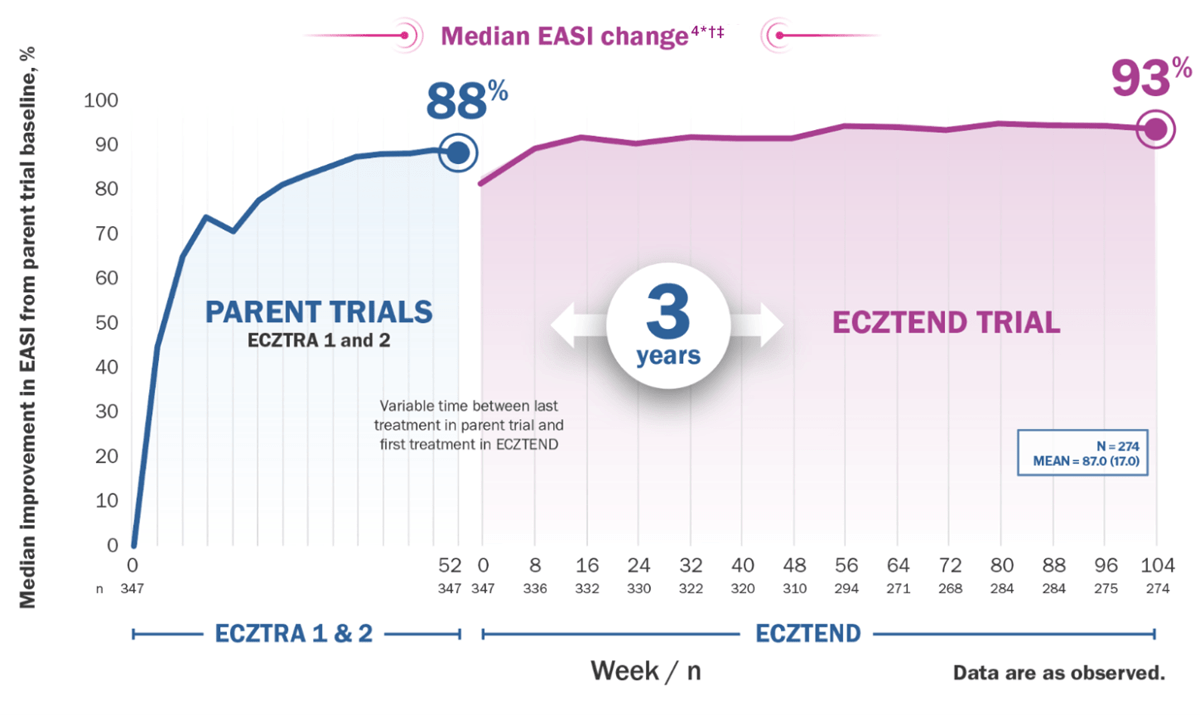
*Median EASI score at parent trial baseline: 26.7; at ECZTEND baseline: 4.7; at Week 104: 2.0.
†Variable time between last treatment in parent trial and first treatment in ECZTEND (maximum 26 weeks).
‡A total of 1430 patients were enrolled in ECZTEND at data cutoff. Data presented from a post-hoc interim analysis of an ongoing OLE trial represents a selected subgroup of patients (n=274) who were eligible, chose to enter from 2 of the parent trials (ECZTRA 1 and ECZTRA 2), and were treated for 3 years by the time of data cutoff (April 30, 2021), and as such, the data may not be generalizable to the full Adbry population.
Limitations:
Limitations and context associated with the open-label study design and data are described above and include decreasing sample size, potential continued involvement of responders, and attrition of nonresponders. Data presented are descriptive in nature and no statistical comparisons are made
Long-term safety with Adbry for up to 3.5 years was generally similar to the parent trials’ initial treatment period with respect to overall frequency of most common AEs (≥5.0%): viral upper respiratory tract infection* (20.6%); atopic dermatitis (18.0%); upper respiratory tract infection (7.1%); headache (5.0%); conjunctivitis (5.3%)3
*Most commonly reported as common cold.